Medically Unlikely Edits (MUEs): Unlikely, But Not Always Impossible
2019-10-18
Medically Unlikely Edits (MUEs) were created by the Centers for Medicare & Medicaid Services (CMS) to help lower the error rate for paid Part B claims. MUEs are the maximum units of a HCPCS or CPT code that a provider would bill under most circumstances for the same patient on the same day. If a claim contains a line item in which the MUE is exceeded, then the line item is denied. The MUE value assigned to codes, based on claims data, is designed to allow the majority of appropriately coded claims to pass the edit. The MUE tables are published on the CMS MUE webpage: www.cms.gov/medicare/coding/
The tables are updated quarterly, so the date of service will need to be considered. It should be noted that not all HCPCS/CPT codes are assigned MUEs, and some codes that have MUEs are not published in an effort to curtail the potential for abuse. In the early days of implementing MUEs, physicians might have been overheard asking, "How many units will Medicare cover for a certain service?", or a biller might think there was no recourse for a claim denial based on MUEs. CMS, however, did not intend to put strict limits in place on all codes. In addition to finding the value for units of service for codes in the MUE tables, there is an additional column to the right that assigns an MUE Adjudication Indicator (MAI) to the code.
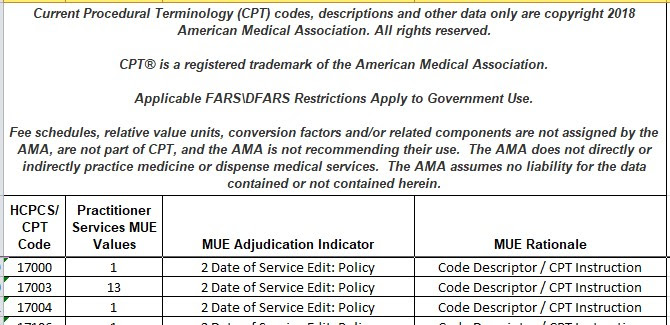
The MAI is the logic behind the edit. The adjudication indicator values are 1, 2, and 3. Most codes that have edits are either MAI 2 or 3. MAI 2 is a date-of-service edit and is absolute. These denials cannot be appealed, because justification would be impossible (e.g., an appendectomy would have an MUE of 1 and MAI of 2). The maximum units billable for an appendectomy is one, because a patient only has one appendix. While the prior example shows how MAI 2 prohibits billing the medically impossible, MAI 2 might also help avoid an error that is systematically impossible (e.g., CPT code 17000 used for lesion destruction states in the definition "first lesion"). By definition, it would be impossible to bill anything other than one unit of service. Additional units of service for lesion destruction would be billed with the add-on code +17003 or code 17004.
Codes with MAI 3, on the other hand, are what coders and billers need to thoroughly understand. Remember that the MUEs listed for a code are based on what would allow most claims to pass. With MAI 3, exceeding the units of service listed in the edit is unlikely but not impossible. MAI 3 indicates that a denial could be appealed. Billers who are well-versed in the codes they commonly bill (and any MUE limits associated with those codes) could avoid a denial by splitting the code up onto multiple line items with an appropriate modifier - e.g. modifier 59 or modifier 76 (in order to individually bypass the edit upon the claim's initial submission). For claims that are accidentally submitted with excess units of service, the provider/billing staff would need to appeal denials and present medical records justifying the units that are in excess of the edit. When a claim is denied for MUEs, the tables should be consulted to see which indicator is assigned to the code. If the indicator is MAI 3, then the claim needs to be appealed and the provider should expect payment.
In summary: Do not fall prey to the notion that an MUE denial is final or absolute. Consult the MUE tables, and appeal denials whenever it is justified. Remember that the edits are to indicate when the units of service exceed what is likely but not always what is impossible.